
Connecticut Harm Reduction Alliance (CTHRA) (formerly known as the Greater Hartford Harm Reduction Coalition) is a non-profit organization based in Hartford, Connecticut, whose mission is to promote the dignity and well-being of individuals and communities impacted by drug use through through the provision of health education and tiered risk reduction programs.
Since the Covid-19 outbreak began, CTHRA and Trek Medics have been working together to reduce fatal opioid-related overdoses in Hartford through a community-based overdose response network that sends simple text messages to community responders equipped with naloxone when an active overdose is reported.
Within the first 30 days of the program, CTHRA staff responded to over 60 overdoses, arriving on-scene on average in less than 6 minutes — and very often before formal emergency responders.
We sat down with CTHRA’s founder and executive director, Mark Jenkins, to hear what he had to say about the opioid epidemic, the impact of Covid-19, and the role of communities in responding to overdoses.

What is “Harm Reduction”?
“Harm Reduction is a set of principles and strategies to help reduce the negative effects of illicit drug use. But it’s much more than that. It’s a credo that every one of our staff and volunteers share, to create a positive impact on the people in our community who are adversely affected by illicit substance use. We’re here to assist our participants and promote positive change in people’s lives, however small that change is.
“I tell this to our team all the time: As an Ambassador we all have the same job description which is; (1) go out into the communities we serve and find out what people need to reduce risk. (2) Get them what they need. (3) Show up tomorrow and do the same thing again. And most importantly, (4) Don’t be an asshole.
“For many individuals we serve, we may be the only people they’ll encounter in a day that they’ll see as a ‘friendly’ — non-judgmental, non-coercive. All we want to know is, ‘What do you need? How can we help?’ Our job is to help people stay safe, regardless of the activity.”
How did the Connecticut Harm Reduction Alliance start?
“Out of frustration, resentment and necessity, really, and not necessarily in that order — knowing that there was a need to be met and the people who were tasked with meeting those needs weren’t doing it. I said, ‘I can do this myself.’ I knew enough people, had already been doing the work locally over a dozen years. So I put together a board, found a lawyer to help us get our 501(c)3, got a bookkeeper, office space and the agency was born in 2014.
“Since those humble beginnings we’ve put together probably Connecticut’s leading harm reduction organization — definitely the state’s only harm reduction organization by mission, vision and values. We’re the state’s largest hand-to-hand distributor of naloxone, and we run the largest web of street outreach workers in the state, working in Hartford, East Hartford, Torrington, Enfield, New Britain, Bristol, New Haven, Manchester and Meriden.”
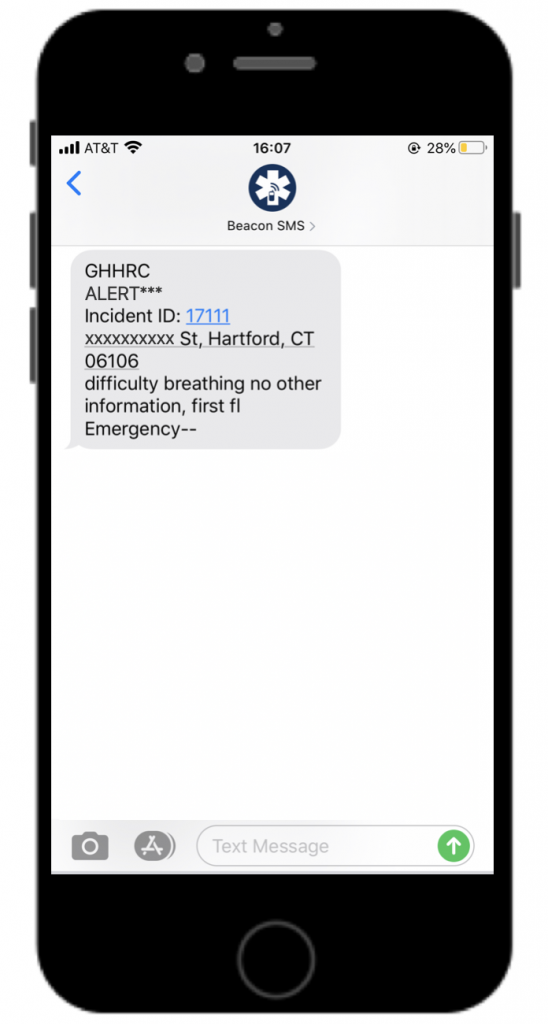
At this point in the interview, Mark was interrupted by a text message.
- Mark: “I think the Beacon alert just went off.”
- Jason: “Do I need to let you go?“
- Mark: “No, we got our people out in the vans. They’ll get there.“
How does this all work? Your staff finds out about an overdose, you send out text messages, and…?
“Yes, exactly. We have about 13 outreach workers who are all trained and equipped with various types of naloxone. And they’re out on the streets every day, either in our RV or in one of our two minivans. The RV has scheduled stops where they go to do street outreach. The minivans, when they’re on duty, they have flags on the back of vehicles so people know who they are, and they do unscheduled stops in all our communities, checking on people, making sure they’ve got what they need to stay safe — and since COVID broke out, they’ve been giving out food and masks and PPE — and people can wave them down, just like it was a Mr. Softee or a Good Humor truck, except they’re getting access to clean syringes, naloxone and safer sex kits. And they also give out our bracelets, to remind them whom to call when they see an overdose.
“So they’re out on the streets every day, doing their job. Tani, our office manager has the office cellphone and she takes calls and listens to the Fire Department scanner, too. And when people call us to report an overdose, we call 911 to report it for them — because people don’t always want to call 911 — and then we use Beacon to send out alerts to all our street outreach teams to find out who’s closest. If we hear something go out on the radio, we do the same thing.
“When any of our team gets there on scene, and they find the person unresponsive, they get to work: They shake that person, do a sternal rub, if they’re blue in the face, they do rescue breathing, and they get out their naloxone and administer it. I always tell them, ‘When in doubt give it; it’s not harmful.’ If you give naloxone, and that person didn’t overdose on opioids, it’s not going to hurt them.”
Some people might think this sounds a little unsafe.
“There’s nothing unsafe about it. We’re not strangers in our communities. A lot of people that work with us are gatekeepers in their community. And we’re providing a service that people are grateful for. We have a positive experience with the people we serve as much as we have a positive experience with the formal responders. And we’re calling 911, too, always. We don’t want to be out there trying to do it on our own. We want to be a value-add to the 911 system. If we get on scene first, we get to work. If police or fire or EMS gets on scene first, we are present to be a resource. We likely know that person, while the first responders may not, so we’re a friendly face that person will recognize.
“All we’re doing is sending community members back into their communities — and we’re arming them with tools and education. We’re not only welcome in these communities; we’re often the only familiar faces to them. And now first responders are welcoming us. We leave naloxone or PPE on scene for the individuals, and we leave it with the police, and with EMS, too, because sometimes they don’t even have it themselves.”

You’re working in the inner city, handing out bracelets to black and brown folks that say “Don’t Run, Call 911”. Is that a hard case to make with all that’s been going on?

“The 911 service is our uniform system for emergency response in the US — like it, love it, hate it, leave it. I don’t have feelings either way. We’re trying to save lives. We’re trying to get people to think above that and remove those barriers — be it fear, anger or what have you.
“It’s our job to be ambassadors of goodwill on both sides — whether it’s ambassadors of goodwill to those we serve or to the police.
“Today was just another case in point where we responded to yet another overdose and even though police and EMS were on scene before us, we were allowed to leave naloxone with the person that overdosed. Once those individuals are in the care of police and EMS, they don’t have to give us access to the individual, but they do.
“Here’s another story: A couple weeks ago, two of our outreach workers, Annie and Alixe, got on scene of an overdose and they saw that the patient was already turning blue and had snoring respirations so Annie administered a dose of naloxone and began rescue breathing. After a couple minutes, the patient wasn’t responding so Alixe handed over a dose of naloxone and she administered a second dose. At this point fire and police show up. They saw that our team had things under control and they stood back and let our people do their thing. Soon after, the patient was revived and when EMS arrived, they let the patient leave. Afterwards, police and fire were talking with Alixe and they told her how impressed they were with how well Annie handled the situation. They said to her: ‘She was so calm and caring. She knew exactly what to do. What training does she have?‘. Alixe just shrugged, ‘She only has naloxone training — and she’s a kind person. She’s already reversed over a hundred overdoses herself and we just want to keep doing this because it means people can get help quicker and it also takes some of the pressure off of you.’ The cops and firefighters were fully impressed and even gave her a pat on the back. It’s not everyday that the fire department is going to give you a pat on the back. That really meant a lot to all of us — and those girls were smiling for two days straight.
“Regardless of my personal feelings, there’s a bigger picture at hand: We need to save lives and reduce barriers to other people calling 911. Let’s work together. If we gotta hold hands and skip down the street with first responders to get people to call 911, let me get on my skipping shoes.”

“Opioid Epidemic”
“Needless, unnecessary death. That has been the over-arching monologue for this epidemic — unnecessary fatalities. And our answer, CTHRA’s resolve in the face of the unrelenting amount of fatalities has been to just keeping showing up, just be a constant presence. Whether it’s in the communities we serve or in the higher halls of power, like the ADPC [Alcohol and Drug Policy Council], various opioid working groups, health fairs and town halls, we’re showing up and we’re having the difficult conversations and even being the one to breach the difficult conversations. It’s just through that dogged persistence of being present as a credible source of information and deliverer of services — people have taken notice, agencies have taken notice.
“The difficult conversations, from the early facts that it didn’t become an epidemic until white people started dying; not until it crossed over Avon Mountain or hit Hyannis that it became an epidemic. As long as it was in the inner city, it was business as usual. Or, the continued increase in overdose fatalities, the necessary actions to prevent and reduce overdose fatalities, these are the conversations we present. Yet those in power still don’t want to have these conversations and ultimately seem to hope this (or maybe us) will go away. Unfortunately, the numbers continue to rise. We’ll see them rise again this year because we aren’t willing to do what’s needed. Our [country’s] response to this epidemic has been piecemeal. People want to test the waters first. We find ourselves slowly trying new things and slower yet to adopt things that work. Look at naloxone: This medication has always worked, and it’s never been harmful, yet only in the past couple of years has it become readily available at the layperson level. We have increased access to MAT [medication-assisted treatment, e.g., Methadone], but that’s still too taboo. And no way does anyone want to breach the subject of safe consumption spaces, ‘uhh… no thanks.’
“The truth is that substance use/disorders are still seen as a moral problem. In harm reduction we’re already used to epidemics because we were born out of the HIV epidemic. We’ve been here before. When responding to public health crisis, the strategies which work the best are often the least tolerable because they tend to offend the morals of Mr. and Mrs. John Q. Public.
Unfortunately we’re going to keep seeing increases in fatalities because our illicit drug supply has changed, forever — it’s not going back to what it was. Fent’s here and it’s not going away. It’s a difficult drug in that it’s unpredictable, the dosing is dangerous, it’s Russian roulette because it’s such a short-acting drug. Heroin last 6-8 hours, Fent lasts 1-2 hours and that’s just good for business — it’s cheaper, more potent and the high doesn’t last as long. In the end it’s all business. Would you rather have a person come to you with $30 once a day or $30 three times a day?
The first rule in business is marketing — and this plays into who we are as a country. The US has an insatiable need, a proclivity for instant gratification, for an instant fix. When you go into a doc’s office, the first question you’re asked during triage is about your pain index. ‘What’s your pain on a scale of 1-10?‘. It may be 3, but you’re going to say 7, and not because you’re going to get a lollipop, because you’re going to get a prescription. You may not even need or want to use it now so you put it in your medicine cabinet, ‘just in case‘. Well, 4 out of 5 people who presently suffer from SUD [substance use disorder] got their drugs from someone they know and more often than not it’s from their medicine cabinet. This all started with prescription drugs. And the VA [Veteran’s Affairs, the US military health service] was one of the early culprits. As a young vet with a shoulder injury, the VA prescribed me 90-day supplies of Perc at a time.
“Prescribing is another place where race played a huge part in this epidemic. The epidemic has disproportionately affected black and brown people, but we were spared from the front end prescription problems because doctors were much more willing to give a prescription to a white person than a minority, simply because they believed the minority person would sell their prescription medication.”
Where is the country headed in this epidemic?
“We are going to see some change, but NIMBY [“Not in my backyard”] is alive and well in this state as well as in others. Most of the public health responses that work offend people, and as such, it makes progress that much harder. NIMBY is just as strong in minority communities as it is in white communities.
“Since 2015 CTHRA has had the longest-running Overdose prevention training and Naloxone distribution program in the state [of Connecticut]. In total, we’ve given out more than 10,000 naloxone kits. Depending on the kit, there are 2-3 doses in each, so we’ve easily given out more than 20,000 doses. Even now our outreach kit numbers have surpassed 7,500 and that’s not counting any of the naloxone we’ve given to other communities around Hartford. The weekly trainings account for 40% of what we have distributed and 75% of the people that attended those in-house trainings have been from white communities, which led to concentrated efforts to do more trainings in other community settings. With the onset of COVID-19 group trainings have gone to the Zoom platform but 1-on-1 trainings with our participants have skyrocketed and we’re back to giving out way more naloxone on the street. We’re also giving out food now, along with PPE kits, because the need for food, and prevention items like face masks, PPE and other resources have increased as a result of Covid-19 while those offering services have decreased.
“So now we’re fighting two epidemics, fatal opioid overdose and Covid-19. We’ve increased our street outreach by adding more personnel and alternating work days and mobile units, thereby keeping an increased presence on the streets while minimizing staff exposure. The safety of our staff and participants is our top priority. Covid-19 is just the latest obstacle we face, overdoses haven’t stopped and when the urgency of the Coronavirus is over we will still be facing the challenges associated with illicit substance use, addiction and overdose fatalities.
To learn more about the Connecticut Harm Reduction Alliance’s pioneering work protecting and saving lives, please visit their website at:
www.ghhrc.org
To learn more about how Trek Medics helps communities prevent fatal opioid overdoses through our Beacon dispatch platform, visit:
www.trekmedics.org/beacon/overdose/
Support from Our Partners
Disaster Technology Grant Awardee
Impact Fund Awardee 2017 & 2019

